By Marilia Coutinho and Antonio Bruno
The older and more experienced the athlete, the higher the chances of him having accumulated injuries and chronic pain. The paradox here is that at the elite level, the perfect athlete would be the older, genetically and mentally gifted athlete with the young body, or as the saying goes “youth is wasted on the young.” The older, injured athlete in chronic pain, then, cannot afford to be anything less than perfect. Any deviation from perfect technique may trigger a level of pain that will immediately inhibit the motor task at hand, and this is not voluntary. If you see one such athlete, enjoy it while you can.
As in many interesting issues in sports performance, there is much evidence indirectly related to the phenomenon and wide gaps in knowledge. What we do know is that pain inhibits maximal strength and proprioceptive response (Graven-Nielsen et al 2002, Farina et al 2004, Farina et al 2005, Power et al 2016, Gill and Callaghan 1998, Barrett et al 1991). We also know that this inhibition probably happens at the central level (Farina et al 2005).
There is something else we know: pain threshold and tolerance are higher in athletes (Walker 1971, Ryan and Kovacic 1966, Guieu 1992, Scheef 2012). However, actual pain perception is not (Tesarz). How do we account for that? There may or may not be physiological adaptations that result in altered threshold and tolerance (Scheef et al 2012). Other hypotheses are that these phenomena are an acute response to exercise itself (Guieu et al 1992), or a response to an altered emotional or social state (Cohen et al 2010). A recent study showed that athletes lose their advantageous pain modulation when in distress (Geva et al 2016).
It is definitely still a poorly understood phenomenon. We do know that the athlete is responding differently than the non-athlete to the stimuli, we know his pain threshold is higher, we know that when pain is finally triggered there will be maximal strength inhibition and loss of technical precision, but we don’t know how to connect the dots. Not yet.
From the coach’s corner, we know that pain inhibition causes a hit or miss picture. In the strength sports, where we can actually measure “how much”, we observe that this becomes even more of an issue with limit or near-limit weights. As the pain response might be perfectly controlled at 90%, 95% might be just enough to trigger a shut-down response resulting in a missed lift. And this is referred to as hit or miss because there is often no way to find out until we miss.
There is indirect evidence, from non-athletes, that pain affects proprioception, as mentioned. It also affects kinesthetic awareness, a concept long abandoned but never replaced by anything better, which defines the individual’s perception of their body in relation to and moving in the external environment (Hutton 1966). Pain affects the perception of one’s body and movement relative to oneself (for example, the perception of a joint flexion relative to one’s body) and to things in the environment and the space itself (distance of objects relative to one’s body, shapes, etc). In athletic terms, it is catastrophic.
Inhibited proprioception and kinesthetic awareness lead to improper technique, which, in turn creates more acute pain and inhibits the whole gesture. This can not only lead to a missed lift: it greatly increases both the risk of injury or, commonly, either re-injury or making a pre-existing problem worse.
Bottom line: the injured athlete cannot afford :
- Technical mistakes
- Programming imprecisions
- Not doing pre and rehabilitative work. In fact, there is a point where it comprises about half of his training, since the experienced athlete requires shorter and less voluminous training blocks to respond, but needs a lot more work to repair and prevent injury.
Technical mistakes can often be “pushed through” by a lifter whose musculo-skeletal structure is uncompromised. But as our bodies pay the price for our drive to excel, this becomes more and more problematic. A small technical mis-cue that results in a deviation of bar path can not only irritate, but thoroughly compromise the damaged cartilage of an elbow during the bench press, or put extra pressure on a herniated disc in the squat. There are a variety of dooms-day scenarios that all athletes face when we train, and good technique is our primary way to avoid that darkest of days.
Programming imprecisions should not occur, but no one has perfect programming, no matter what they advertise. The key for the injured, aging athlete is caution. Athletes should know that pushing through an injury is not exactly the wisest course, and lifting heavy just because it felt right is not always the best option, particularly at near-limit lifts. Many days this wisdom seems to be little in evidence for all of us: the published research concerning emotional and social factors as determinants of pain tolerance and threshold explains it. However, as Ed Coan said, “you only have so many PR’s, do not waste them on the gym.”
Pre and rehabilitative work take time, and often cause pain, as they are treating injured areas and/or dealing with underlying pathologies. No one likes this. The athlete must learn to differentiate between types of pain, and understand that achieving optimal performance is only done by achieving optimal health – or as close as the athlete can get to it.
Coaching an experienced, elite athlete is difficult because it often becomes more a case of “crisis-management” than programming. When the athlete has improved their technique over tens of thousands of repetitions, knows programming and how the body responds, they must be reminded of the need for caution. No one likes to be told that they are getting older and have injuries that they could have trained around or pushed through ten years before. Some days you must cautiously “apply the brakes” to a speeding train, and hopefully arrive safely at your destination – yet another championship.
References:
Barrett, D. S., A. G. Cobb, and G. Bentley. “Joint proprioception in normal, osteoarthritic and replaced knees.” Bone & Joint Journal 73.1 (1991): 53-56.
Cohen, Emma EA, et al. “Rowers’ high: behavioural synchrony is correlated with elevated pain thresholds.” Biology Letters 6.1 (2010): 106-108.
Farina, Dario, et al. “Effect of experimental muscle pain on motor unit firing rate and conduction velocity.” Journal of neurophysiology 91.3 (2004): 1250-1259.
Farina, Dario, Lars Arendt-Nielsen, and Thomas Graven-Nielsen. “Experimental muscle pain decreases voluntary EMG activity but does not affect the muscle potential evoked by transcutaneous electrical stimulation.” Clinical neurophysiology 116.7 (2005): 1558-1565.
Geva, Nirit, Jens Pruessner, and Ruth Defrin. “Triathletes Lose Their Advantageous Pain Modulation under Acute Psychosocial Stress.” Medicine and science in sports and exercise (2016).
Gill, Karl P., and Michael J. Callaghan. “The measurement of lumbar proprioception in individuals with and without low back pain.” Spine 23.3 (1998): 371-377.
Graven‐Nielsen, Thomas, et al. “Inhibition of maximal voluntary contraction force by experimental muscle pain: a centrally mediated mechanism.” Muscle & nerve 26.5 (2002): 708-712.
Guieu, Régis, et al. “Nociceptive threshold and physical activity.” Canadian Journal of Neurological Sciences/Journal Canadien des Sciences Neurologiques 19.01 (1992): 69-71.
Hutton, Robert S. “Kinesthetic aftereffect, a measure of kinesthetic awareness.” Perceptual and motor skills 23.3 suppl (1966): 1165-1166.
Power, Geoffrey A., et al. “MOTOR UNIT NUMBER AND TRANSMISSION STABILITY IN OCTOGENARIAN WORLD CLASS ATHLETES: CAN AGE-RELATED DEFICITS BE OUTRUN?.” Journal of Applied Physiology (2016): jap-00149.
Ryan, E. Dean, and Charles R. Kovacic. “Pain tolerance and athletic participation.” Perceptual and Motor Skills 22.2 (1966): 383-390.
Scheef, Lukas, et al. “An fMRI study on the acute effects of exercise on pain processing in trained athletes.” PAIN® 153.8 (2012): 1702-1714.
Tesarz, Jonas, et al. “Pain perception in athletes compared to normally active controls: a systematic review with meta-analysis.” Pain 153.6 (2012): 1253-1262.
Walker, June. “Pain and distraction in athletes and non-athletes.” Perceptual and Motor Skills 33.3 suppl (1971): 1187-1190.
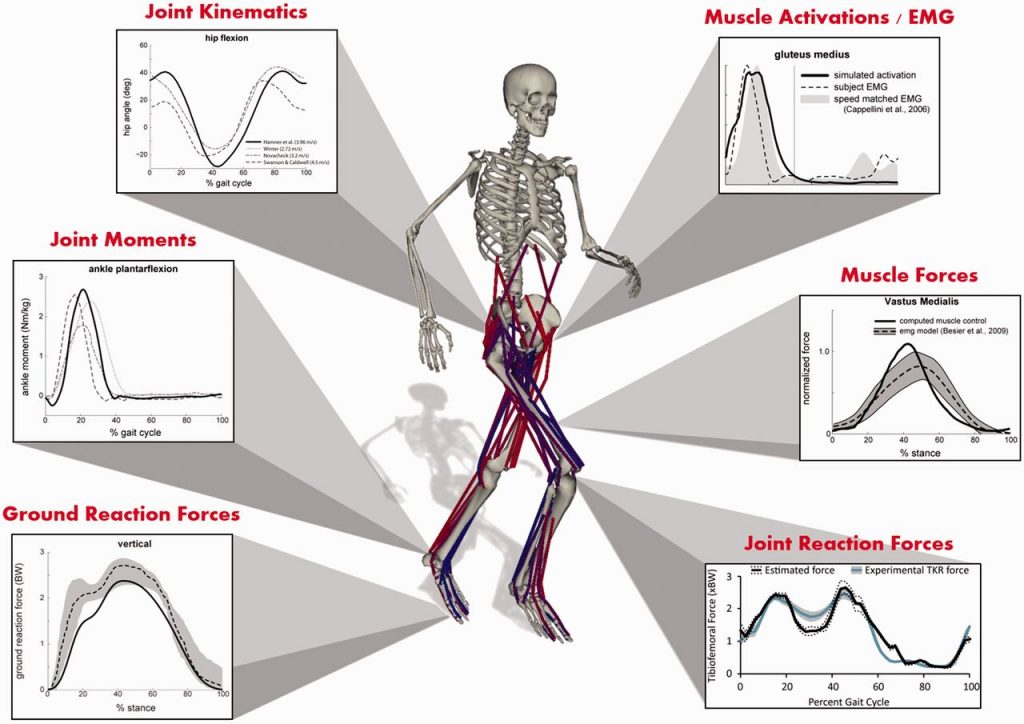
IMAGE: Ku, Joy P., et al. “The Mobilize Center: an NIH big data to knowledge center to advance human movement research and improve mobility.” Journal of the American Medical Informatics Association (2015): ocv071.